Philosophy of Urine Drug Testing in Pain Management
by Howard A. Heit, MD, FACP, FASAM & Douglas L. Gourlay, MD, MSc, FRCPC, FASAM
Expert authors received compensation from Janssen Pharmaceuticals, Inc. for their contributions to Prescribe Responsibly
Urine drug testing (UDT)
Urine drug testing (UDT) is a useful tool in pain management that provides valuable objective information to assist in diagnostic and therapeutic decision making. 36 Results of a UDT provide confirmation of the agreed-upon treatment plan (adherence/compliance). They can diagnose relapse or drug misuse as early as possible, and they also can be used to advocate for the patient with third-party interests.37
To assess compliance, the healthcare professional may look for the presence of prescribed medications in the urine as evidence of their use. Finding no presence of the prescribed drug or finding unprescribed or illicit drugs in the urine merits further discussion with the patient. At the same time, it is important to recognize that laboratory error and test insensitivity can result in misleading data. Bingeing by the patient can result in unexpected negative urine reports if the patient runs out of medication prior to urine sample collection. Therefore, these results by themselves cannot be relied upon to prove drug diversion and may be consistent with
addiction, or the use of an opioid for non-pain purposes—so called chemical coping.36
The purpose of UDT should be explained to the patient at the initial evaluation. UDT can also enhance the relationship between healthcare professionals and patients by providing documentation of adherence to mutually agreed-upon treatment plans.
36
In the pain management setting, the presence of an illicit or unprescribed drug does not necessarily negate the legitimacy of the patient’s pain complaints, but it may suggest a concurrent disorder such as
drug abuse or addiction. The patient must be willing to accept assessment and treatment of both disorders to receive adequate outcomes in either. Thus, the diagnosis of a concurrent addictive disorder, when it exists, does nothing to negate a legitimate pain disorder; rather, it complicates it.36
Specimen Choice
Urine has been the preferred biologic specimen for determining the presence or absence of most drugs. This is, in part, due to the increased window of detection of 1 to 3 days for most drugs and/or their metabolites.
36
Whom to Test and Frequency of Testing
The question of whom to test is made easier by having a uniform practice policy either in a pain or primary practice that would help reduce individual stigma. Any risk of patient profiling based on
racial, cultural, or other physical appearances is eliminated. Careful explanation of the purpose of testing normally allays patient concerns. 36
Healthcare professionals sometime find the subject of drug testing a difficult one to explore with their patients, especially those who have been in the practice for many years. Often, a healthcare professional's perception is that requesting a urine sample for drug testing may be seen as mistrusting the patient and, consequently, potentially damaging to the healthcare professional-patient relationship. In fact, when approached in a respectful, patient-centered fashion, most patients are more than willing to do their part in managing risk in order to receive the care that they need.
Testing Strategies
The healthcare professional must know the drugs for which to test, appropriate methods to use, and the expected use of the results obtained.
36 Immunoassay drug tests are most commonly used. They are designed to classify substances as either present or absent and are generally highly sensitive. In pain management, specific drug identification using more sophisticated identification tests is needed.36 Techniques such as Gas Chromatography/Mass Spectroscopy (GC/MS) and High Performance Liquid Chromatography (HPLC) are used for the identification of a specific drug and/or its metabolites.36
Immunoassay drug tests for natural opiates are very responsive to morphine and codeine, but do not distinguish between the two. UDT by immunoassay also shows a low sensitivity for semisynthetic/synthetic opioids such as oxycodone and fentanyl.
36 Even though an immunoassay may be negative for consumed oxycodone, it should be positive on GC/MS if the drug was used within the window of detection. The clinical importance of this fact with UDT cannot be overstated, because compliant patients may have been dismissed from pain management practices secondary to a false-negative immunoassay test when looking specifically for prescribed oxycodone.36 Specific drug identification by chromatographic testing (ie, GC/MS) also is necessary to identify which member of the detected class is responsible for the positive screen.36 Drug-specific immunoassays presently on the market and under development will identify semisynthetic/synthetic opioids.37 The healthcare professional should always know the limits of the UDT ordered.37
A routine UDT screening panel suggested for the following drugs/drug classes is listed in Table 4.36
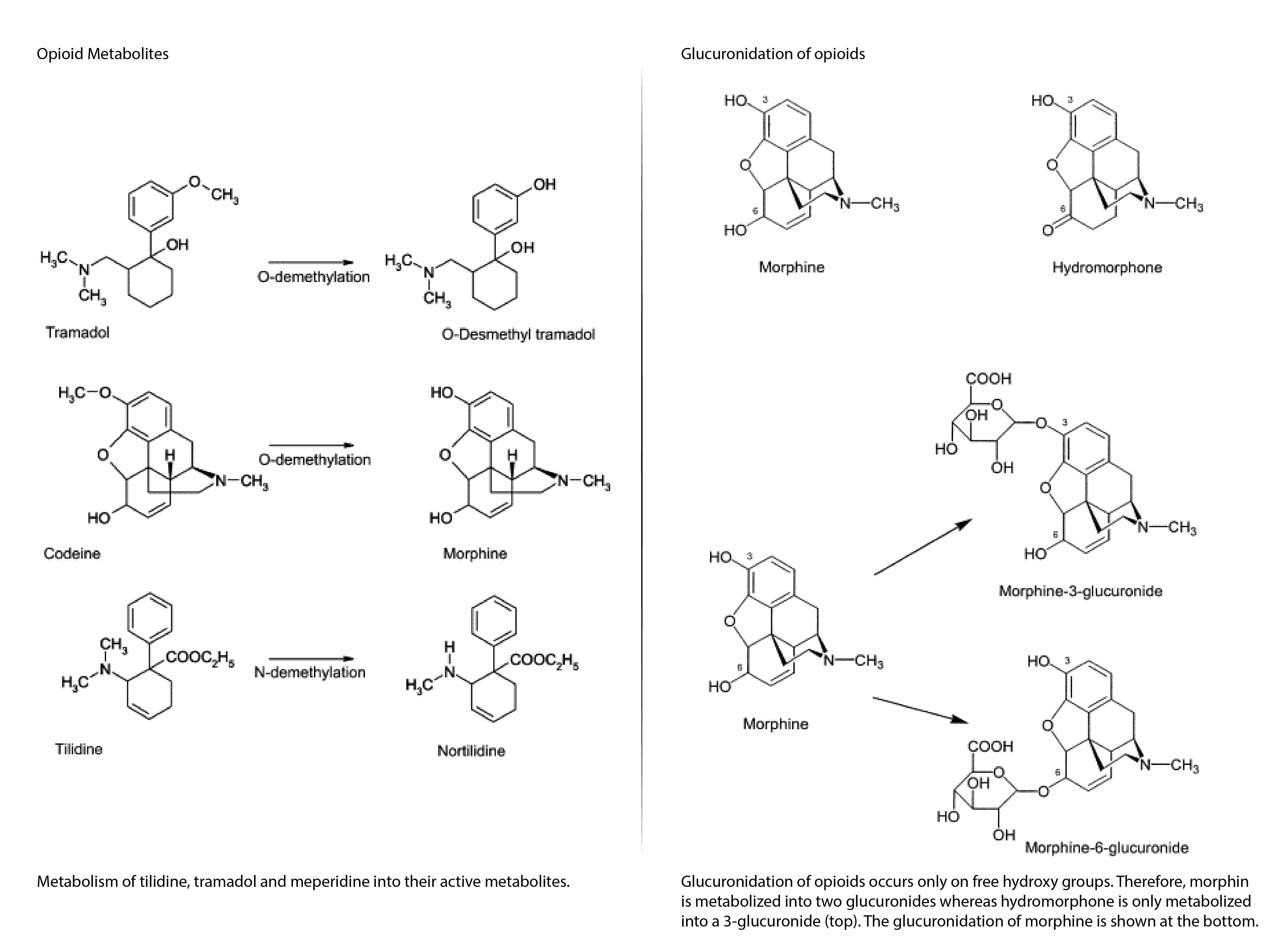
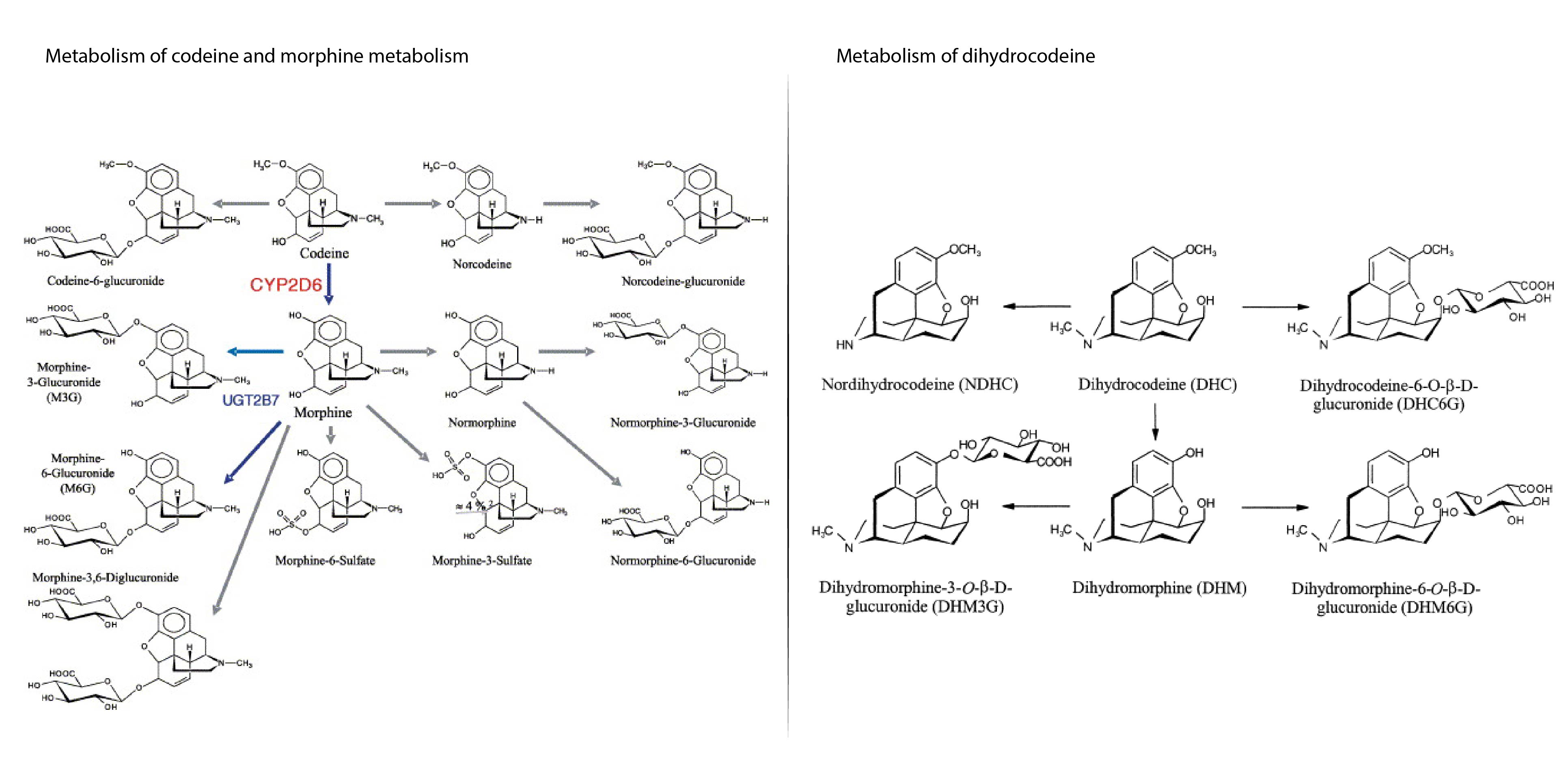
Healthcare professionals also must understand the basic metabolism of commonly prescribed drugs, especially opioids, so they will be able to explain a UDT result that is positive for the prescribed medication and/or its metabolite(s).
Dealing With Unexpected Urine Toxicology Results
UDT in clinical practice must be used to improve patient care. Unfortunately, these test results may come back unexpectedly negative for a prescribed drug or positive for an unprescribed one. The first step in interpreting these results is to contact the lab to ensure that no clerical errors have been made.
37 If unexpected results are confirmed, there must be a process in place that should include discussing the unexpected result with the patient.36
Conclusion
UDT is an effective tool in the assessment and ongoing management of patients who will be, or are being, treated chronically with controlled substances. Most importantly, a healthcare professional should have a relationship of mutual honesty and trust with the patient when using UDT in the clinical practice, as well as maintain open communication with the testing laboratory. The use of UDT should be consensual; it is designed to improve patient care and to assist the healthcare professional to advocate on the patient’s behalf.
36
TABLE 3: Windows of Detection in Urine Drug Testing36
Drug
Approximate Retention Time
Amphetamines
48 hours
Barbiturates
Short acting (eg, secobarbital): 24 hours
Long acting (eg, phenobarbital): 2-3 weeks
Benzodiazepines
3 days, if therapeutic dose is ingested
Up to 4-6 weeks after extended dosage (ie, 1 or more years)
Cocaine
Metabolite
2-4 days
Ethanol
2-4 hours
Methadone
Approximately 3 days
Opiates
2 days
Propoxyphene
6-48 hours
Cannabinoids
Moderate smoker (4 times/week): 5 days
Heavy smoker (smoking daily): 10 days
Retention time for chronic smokers may be 20-28 days
Phencyclidine
Approximately 8 days
Chronic users: up to 30 days
(mean value = 14 days)
Note: Interpretation of retention time must take into account variability of urine specimens, drug metabolism and half-life, patient's physical condition, fluid intake, and method and frequency of ingestion. These are general guidelines only.
TABLE 4: Suggested Screening Panel36
A routine UDT screening panel should test for the following drugs/drug classes:
Cocaine
Amphetamines/Methamphetamine
Opioids
Methadone
Marijuana
Benzodiazepines
Metabolism of Opioids37
References Used in the Section:
36 Heit HA, Gourlay DL. Urine Drug Testing in Pain Medicine. The Journal of Pain and Symptom Management. 2004; 27(3):260-267.
37 Gourlay D, Heit H, Caplan Y. Urine Drug Testing in Primary Care: dispelling the myths & designing strategies. Monograph for California Academy of Family Physicians. 2006.
Diagrams